
Calcifying Epithelioma (Pilomatrixoma) Treatment | IC Clinic Shinjuku
“I have an unexplained lump on my body and don’t know what to do.”
“I want to see a doctor, but I’m not sure which specialty to visit.”
If you have a growth on your skin, it may be a calcifying epithelioma.
Calcifying epithelioma is a benign subcutaneous tumor in which a portion of the skin hardens like calcified tissue. It does not resolve on its own, and attempting to manage it yourself carries the risk of worsening the condition, so please consider visiting a clinic.
This page explains the causes, characteristics, and treatment options for calcifying epithelioma. If you are troubled by a skin growth, we hope you will find this information helpful.
What Is Calcifying Epithelioma? A Hard, Stone-Like Lump of Unknown Cause

The exact cause of calcifying epithelioma is not yet fully understood; it is a type of benign subcutaneous tumor in which part of the skin hardens like calcified tissue [1,3].
Formally known as “pilomatrixoma,” it is a relatively rare skin tumor first reported by Malherbe in 1880 [3,19].
As the alternative name “pilomatrixoma” suggests, it originates from hair follicles, and mutations in the β-catenin gene—which plays an important role in hair differentiation—have been reported [5,7,8].
Activating mutations in the CTNNB1 gene (β-catenin) are found in approximately 90% of cases, and abnormal activation of the Wnt signaling pathway is considered to be the underlying cause [5,7].
The lumps associated with calcifying epithelioma tend to develop most often in individuals aged 20 or younger, and females appear to be somewhat more frequently affected [4,10,11].
Large-scale epidemiological studies indicate that approximately 60% of patients are aged 20 or younger, with a male-to-female ratio of approximately 1:1.5, showing a slightly higher prevalence in females [4,11,18].
The overall incidence is estimated at approximately 1–2 cases per 100,000 people per year [18].
Calcifying epithelioma most commonly appears on the face, neck, and arms.
There is generally no familial inheritance (although multiple lesions on the head may be hereditary and can be associated with myotonic dystrophy) [14].
In patients with myotonic dystrophy type 1, multiple pilomatrixomas are reported to occur at approximately 10 to 20 times the frequency seen in the general population [14].
Symptoms of Calcifying Epithelioma
The condition tends to occur most often in younger individuals aged 20 or under, with a slight female predominance.
Common sites of occurrence include the face, neck, and upper limbs.
When calcifying epithelioma develops, a hard, stone-like lump can be felt beneath the skin.
Most cases are asymptomatic, although tenderness (pain when pressed) may sometimes be present. The color is usually similar to the surrounding skin, but if the tumor beneath is visible through the skin, it may appear bluish-black.
The surface of the tumor is irregular, and it can be moved beneath the skin when gentle pressure is applied.
Malignant tumors are also often hard and irregular on the surface, but unlike calcifying epithelioma, they typically do not move when pressed from outside. A key distinction is that calcifying epithelioma is mobile beneath the skin, whereas malignant tumors generally are not.
However, calcifying epitheliomas that are exceptionally large or have limited mobility can sometimes be difficult to distinguish from malignant tumors.
Calcifying Epithelioma Can Be Diagnosed Using CT or MRI

Diagnosis of calcifying epithelioma does not begin with advanced testing; the affected area is first assessed through visual inspection and palpation.
In some cases, an ultrasound examination is sufficient for diagnosis. X-ray imaging can also help identify the location of the tumor and support a diagnosis of calcifying epithelioma, but in early stages before significant progression, the findings may not yet appear clearly on imaging.
For a more accurate diagnosis, CT scanning (which uses X-rays to capture cross-sectional images of the body) or MRI (which uses powerful magnets and radio waves to produce internal images) may be used [6,25].
CT imaging typically reveals characteristic eggshell-like calcification, while MRI shows mixed signals on both T1- and T2-weighted images—findings that are considered hallmarks of this condition [6].
By imaging the entire body to assess the location and relationship of the tumor, these methods help improve diagnostic accuracy.
CT and MRI also make it possible to distinguish calcifying epithelioma from other conditions that may be difficult to identify by appearance alone.
Histopathological Features
Histopathologically, the three characteristic hallmarks are basophilic cells resembling hair matrix cells, eosinophilic shadow cells, and calcification [2,3,19].
Immunohistochemically, nuclear accumulation of β-catenin protein is a key diagnostic finding [5,8].
In the pathological diagnosis of pilomatrixoma, the triad of basophilic hair matrix-like cells, shadow cells, and calcification is of primary importance [2,3,19].
Immunohistochemically, nuclear accumulation of β-catenin is essential for confirming the diagnosis and is useful in differentiating the condition from other skin tumors [5,8].
A pattern of CD34 positivity and cytokeratin negativity is also recognized as a characteristic finding [19].
Quantifying the Risk of Malignant Transformation
Malignant transformation of pilomatrixoma (pilomatrix carcinoma) is extremely rare, occurring in approximately 0.5–2% of all cases [21,22].
Malignant transformation is typically seen in cases with multiple lesions or large tumors that have been left untreated for an extended period; rapid growth and ulceration are warning signs [21,22].
Epidemiology and Incidence of Pilomatrixoma
Pilomatrixoma is a relatively rare skin tumor, accounting for approximately 0.5–1% of all skin tumors [18].
The annual incidence is estimated at approximately 1–2 cases per 100,000 people, with the highest occurrence from childhood through adolescence [10,11,18].
The head and neck region accounts for approximately 70% of cases, followed by the upper limbs and trunk [12,15].
Molecular Biology of Pilomatrixoma
Abnormal activation of the Wnt signaling pathway plays a central role in the pathogenesis of pilomatrixoma [5,7,8].
Activating mutations in exon 3 of the CTNNB1 gene are found in approximately 90% of cases, and abnormal accumulation of β-catenin protein leads to impaired differentiation of hair matrix cells [5,7].
These molecular biology findings provide important insights for improving diagnostic and therapeutic strategies [8].
Post-Treatment Course and Long-Term Prognosis
With appropriate surgical excision, the prognosis is generally favorable, with recurrence rates below 1% following complete removal [17,18].
Cosmetic satisfaction after surgery is also generally high, and scars tend to become less noticeable over time [6,25].
However, in cases associated with myotonic dystrophy, where multiple lesions tend to develop, long-term follow-up is recommended [14].
Pilomatrixoma and β-Catenin
Molecular biological research on pilomatrixoma has attracted significant international attention, and the discovery of β-catenin gene mutations was a landmark finding [5].
How Is Calcifying Epithelioma Different from an Epidermoid Cyst? Distinguishing It from Similar Tumors

The following conditions can appear similar to calcifying epithelioma:
| Condition | Characteristics |
|---|---|
| Epidermoid Cyst (Atheroma) | Gradually enlarges over time |
| Lipoma | Develops primarily in the subcutaneous fat layer |
| Steatocystoma | Once formed, tends to appear in multiple locations |
Below, we explain how to distinguish calcifying epithelioma from similar conditions. Since the appropriate approach differs depending on the diagnosis, please use this information as a reference when assessing your own symptoms.
Epidermoid Cyst (Atheroma)
An epidermoid cyst is a tumor in which a lump beneath the skin gradually enlarges over time.
It begins as a small, pouch-like structure that slowly grows as keratin and sebum accumulate inside. Because it produces a subcutaneous lump similar to that of calcifying epithelioma, it can be difficult to distinguish between the two.
If bacteria enter through a small opening on the surface of the cyst and cause infection, symptoms such as pain and redness may develop. In advanced cases, pus may discharge from the affected area, so prompt attention is advisable if an epidermoid cyst is suspected.
For information on the causes and treatment of epidermoid cysts, please visit the following page.
About Epidermoid Cysts (Atheroma)
Lipoma
A lipoma is a condition in which fat-storing cells proliferate, causing a bulge or lump in the skin.
Lipomas can range widely in size, from approximately 1 cm to 10 cm, but they are generally not painful. Most lipomas develop in the subcutaneous fat layer, which forms the deepest layer of the skin. Like calcifying epithelioma, they typically cause no visible changes to the skin surface, making self-diagnosis difficult.
The detailed cause of lipomas has not yet been clearly established. However, since chromosomal abnormalities are observed in close to 80% of lipomas, genetic factors are thought to play a role in their development.
Lipomas tend to grow over time and typically require surgical removal. For information on types of lipomas and the treatment process, please visit the following page.
Steatocystoma
A steatocystoma is a lump that appears around the sebaceous glands, which produce sebum. It typically develops on the chest, underarms, or neck.
Steatocystomas are generally asymptomatic. If the cyst ruptures and becomes inflamed, pain and swelling may occur.
A notable feature of steatocystomas is their tendency to appear in multiple locations once they develop. While surgical removal is performed to treat the condition, there is a risk of recurrence if the cyst itself is not completely excised.
For information on our clinic’s treatment fees for steatocystoma, please visit the following page.
Treatment Options for Calcifying Epithelioma

The treatment for calcifying epithelioma is surgical excision [6,25].
Complete excision can achieve a cure, and when an adequate resection margin is secured, the recurrence rate has been reported to be below 1% [17,18].
Incomplete excision is associated with a recurrence rate of approximately 10–15%, which is why complete removal including the surrounding capsule is important [17].
Calcifying epithelioma tends to grow slowly, but it does not resolve on its own, and bacterial infection can cause the area to become red and swollen.
Oral medications, topical treatments, and laser therapy cannot eliminate the tumor. Therefore, surgical removal is necessary to treat the condition.
Additionally, even if you believe a lump on your body is calcifying epithelioma, there is a possibility that it could be a malignant condition. Since it is difficult to accurately assess symptoms on your own, please consider consulting a clinic if you suspect calcifying epithelioma.
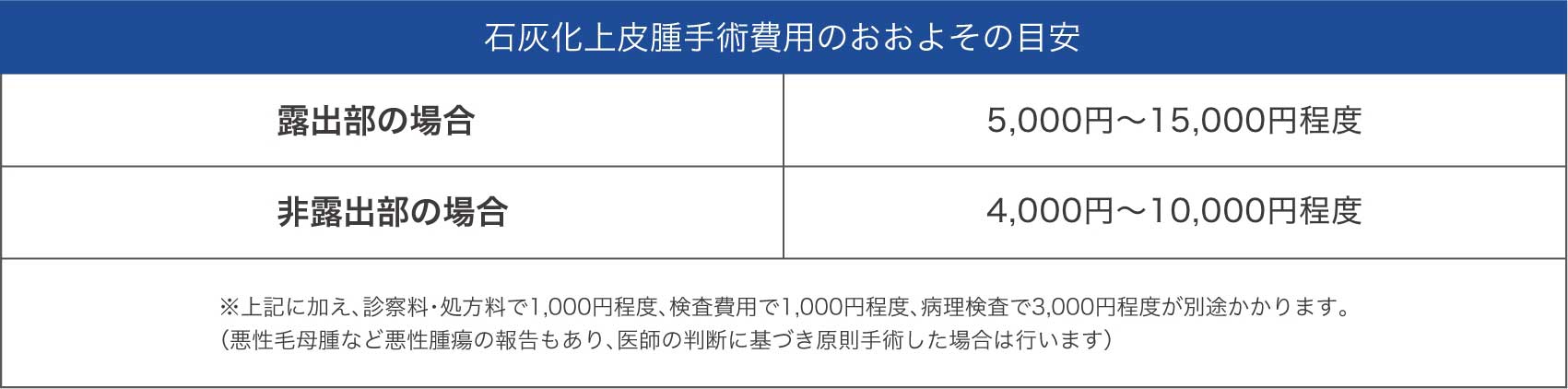
Estimated Cost of Surgery for Calcifying Epithelioma

The approximate cost of surgery for calcifying epithelioma is as follows.
Frequently Asked Questions About Calcifying Epithelioma

Below, we address common questions and concerns about the treatment of calcifying epithelioma.
Please avoid attempting to treat calcifying epithelioma yourself, as this can lead to infection.
Bacterial infection may cause the area to become red and swollen, or the wound may become infected with pus.
In addition, it can be difficult to distinguish calcifying epithelioma from a malignant tumor. To avoid delays in treatment in case what you think is calcifying epithelioma turns out to be malignant, please consider consulting a clinic.
There are mainly two situations in which treatment for calcifying epithelioma may be covered by insurance [6,13].
Coverage applies when malignancy is suspected or when the need for surgery is recognized.
When malignancy is suspected
When the need for surgery is recognized
Under insurance coverage, patients are generally responsible for 30% of the treatment cost. However, treatment for cosmetic purposes is not eligible for insurance coverage.
It is usually a solitary lesion, but it is known to occur in multiple locations in patients with myotonic dystrophy type 1 [14].
In such cases, the incidence is reported to be 10–20 times higher than in the general population, making it an important skin manifestation of this hereditary condition [14].
In most cases, once the lump is surgically removed, recurrence at the same site does not occur.
If you are troubled by multiple calcifying epitheliomas, there is a possibility that you may also have a separate condition called myotonic dystrophy.
Myotonic dystrophy is an inherited disease in which muscle contraction leads to progressive muscle weakness. It can cause tumors to develop in other organs and may lead to calcifying epithelioma of the scalp.
Calcifying epithelioma associated with myotonic dystrophy is characterized by the development of multiple tumors. Since malignant tumors may also occur in myotonic dystrophy, please consult a clinic promptly if you notice any concerning symptoms.
After surgical excision of calcifying epithelioma, a reddish scar will remain, but it tends to fade over time.
The scar may appear as a thin line or slight indentation, and its size will vary depending on the location and size of the tumor.
However, individuals with a keloid tendency—where scars become raised and cord-like—should be aware that their scars may be more noticeable.
Surgery for calcifying epithelioma can be performed on infants and children without any particular issue.
As the condition progresses, the surgical incision required becomes larger, so earlier removal generally leads to a better cosmetic outcome.
Since it is difficult for infants and young children to remain still during surgery, general anesthesia is typically used for patients up to around 12–13 years of age. As calcifying epithelioma is located in the shallow layers of the skin, deep incisions are not required, and the physical burden is relatively limited.
Surgical removal of calcifying epithelioma under general anesthesia in infants and children is not an uncommon procedure, so please do not hesitate to consider an early consultation.
Please note that our clinic does not provide treatment for patients aged 12 or younger. If we receive inquiries regarding infants or children aged 12 or under, we will provide a referral to a general hospital or appropriate facility.
6 Features of Our Clinic That Patients Appreciate
 Team-Based Care Under the supervision of board-certified plastic surgeons certified by the Japanese Society of Plastic and Reconstructive Surgery, our clinic is staffed by specialists from multiple disciplines, including plastic surgery, dermatology, and orthopedic surgery.
Team-Based Care Under the supervision of board-certified plastic surgeons certified by the Japanese Society of Plastic and Reconstructive Surgery, our clinic is staffed by specialists from multiple disciplines, including plastic surgery, dermatology, and orthopedic surgery.
 Attention to Discomfort Our specialist physicians select the most appropriate surgical approach from a wide range of options, aiming to minimize discomfort throughout treatment.
Attention to Discomfort Our specialist physicians select the most appropriate surgical approach from a wide range of options, aiming to minimize discomfort throughout treatment.
 Careful Attention to Scarring We perform surgical excision with great care to avoid damaging the surrounding skin, prioritizing a clean and precise result.
Careful Attention to Scarring We perform surgical excision with great care to avoid damaging the surrounding skin, prioritizing a clean and precise result.
 Insurance Coverage Available At our clinic, treatment may be covered by health insurance when malignancy is suspected or when the need for surgery is recognized.
Insurance Coverage Available At our clinic, treatment may be covered by health insurance when malignancy is suspected or when the need for surgery is recognized.
 No Hospital Stay Required — Same-Day Surgery Available The process from consultation to surgery is smooth and efficient. Same-day surgery is available.
No Hospital Stay Required — Same-Day Surgery Available The process from consultation to surgery is smooth and efficient. Same-day surgery is available.
 Convenient Location We are located just a 3-minute walk from JR Shinjuku South Exit, a major transportation hub in central Tokyo.
Convenient Location We are located just a 3-minute walk from JR Shinjuku South Exit, a major transportation hub in central Tokyo.
Many patients visit our clinic with the following concerns.
Do any of these apply to you?
Patients with an unexplained lump on their body
Patients whose skin has become hard and stone-like in one area
Patients who were told that surgery is possible, but that ultrasound or MRI appointments are not available soon
We will recommend the most suitable treatment approach based on each patient’s individual condition. If you are considering treatment for calcifying epithelioma, please feel free to contact us at any time.
References
- Japanese Dermatological Association, ed. Dermatology, 11th Edition. Bunkodo, 2018.
- Hashimoto K, Brownstein MH, Jakobiec FA. Pilomatrixoma: histochemical and electron microscopic studies. Arch Dermatol. 1974;110(2):209-216.
- Forbis R Jr, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol. 1961;83:606-618.
- Moehlenbeck FW. Pilomatrixoma (calcifying epithelioma): a statistical study. Arch Dermatol. 1973;108(4):532-534.
- Chan EF, Gat U, McNiff JM, Fuchs E. A common human skin tumour is caused by activating mutations in beta-catenin. Nat Genet. 1999;21(4):410-413.
- Japanese Society of Plastic and Reconstructive Surgery, ed. Plastic Surgery, 4th Edition. Kokuseido Publishing, 2017.
- Lazar AJ, Calonje E, Grayson W, et al. Pilomatrix carcinomas contain mutations in CTNNB1, the gene encoding beta-catenin. J Cutan Pathol. 2005;32(2):148-157.
- Hassanein AM, Glanz SM. Beta-catenin expression in benign and malignant pilomatrix neoplasms. Am J Dermatopathol. 2004;26(6):522-524.
- Nariі K, Hashimoto K, eds. NEW Dermatology, 3rd Edition. Nakayama Shoten, 2018.
- Yencha MW, Linfesty R, Blackmon A. Pilomatrixoma of the head and neck in children: a retrospective study. Int J Pediatr Otorhinolaryngol. 2001;57(2):123-128.
- Lan MY, Lan MC, Ho CY, et al. Pilomatrixoma in children: a retrospective study of 179 cases in Taiwan. Arch Otolaryngol Head Neck Surg. 2003;129(10):1109-1112.
- Duflo S, Nicollas R, Roman S, et al. Pilomatrixoma of the head and neck in children: a study of 38 cases and a review of the literature. Arch Otolaryngol Head Neck Surg. 1998;124(11):1239-1242.
- Japanese Dermatological Association. “Clinical Practice Guidelines for Skin Tumors, 2nd Edition,” 2015.
- Aguiar LM, Nico MM, Kamiya H, et al. Multiple pilomatrixomas associated with myotonic dystrophy. J Dermatol. 2004;31(9):729-733.
- Danielson-Cohen A, Lin SJ, Hughes CA, et al. Head and neck pilomatrixoma in children. Arch Otolaryngol Head Neck Surg. 2001;127(12):1481-1483.
- Aničić M, Janković I, Milošević B, et al. Pilomatrixoma: clinical and histopathological study of 149 cases. Arch Dermatol Res. 2012;304(8):649-654.
- Sari N, Yavuzer R, Basterzi Y, et al. Pilomatrixoma in children: experience with 77 cases. Eur J Plast Surg. 2005;28(5):320-323.
- Pirouzmanesh A, Reinisch JF, Gonzalez-Gomez I, et al. Pilomatrixoma: a review of 346 cases. Plast Reconstr Surg. 2003;112(7):1784-1789.
- Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors, 6th Edition. Elsevier, 2014.
- Editorial Committee of the Journal of the Japanese Dermatological Association. “Diagnosis and Treatment of Pilomatrixoma.” Jpn J Dermatol. 2019;129(8):1567-1582.
- Lopansri S, Mihm MC Jr. Pilomatrix carcinoma or calcifying epitheliocarcinoma of Malherbe: a case report and review of literature. Cancer. 1980;45(8):2368-2373.
- Hardisson D, Linares MD, Nistal M. Pilomatrix carcinoma: a clinicopathologic study of six cases and review of the literature. Am J Dermatopathol. 2001;23(5):394-401.
- Brownstein MH, Arluk DJ. Proliferating trichilemmal cyst: a simulant of squamous cell carcinoma. Cancer. 1981;48(5):1207-1214.
- Fletcher CDM, Bridge JA, Hogendoorn PCW, et al. WHO Classification of Tumours of Soft Tissue and Bone, 4th Edition. IARC Press, 2013.
- Robinson JK, Hanke CW, Siegel DM, et al. Surgery of the Skin: Procedural Dermatology, 3rd Edition. Elsevier, 2015.